Surgery
Will I need surgery?
- 25% to 30% of people with ulcerative colitis ultimately need surgery
- Up to 50% of Crohn’s patients will require surgery at some point during their lifetime; however, recent studies have shown a specialist care reduces the need for surgery
Reasons for surgery:
- Medications not working well
- Side effects of medication
- Cancer or increasing risks of cancer
- Severe attacks not responding to medication
- Severe inflammation with perforation/peritonitis
- Severe bleeding
- Strictures of bowel
- Bowel obstruction
- Fistulas (tunnels from bowel to other organs or skin)
- Abscess (boil or collection of pus)
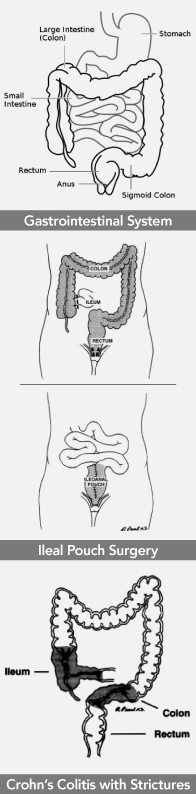
- Ileal Pouch Anal Anastomosis
- J pouch
- S pouch
- W pouch
- Continent Ileostomy
- Permanent Ileostomy
- Ileorectal Anastomosis
Surgery for Crohn’s Disease:
- Segmental Bowel Resection
- Drainage of Abscesses
- Strictureplasty
- Setons
About one fourth to nearly one half of people that have ulcerative colitis will eventually need surgery. Up to 50% of people with Crohn’s disease will require surgery at some point in their lifetime.
Reasons for Surgery:
Sometimes surgery is recommended as a treatment option for IBD when other treatments are not working well or are causing unwanted side effects. People who have had IBD for over 8-10 years have a higher risk of developing colorectal cancer than the general population. Because of this increased risk, patients should have colonoscopy every 1-2 years. A colonoscopy is done frequently to assess the colon by taking biopsies and looking at the biopsies with a microscope. If abnormal cells are found (dysplasia) suggesting a very high risk of colon cancer, surgery may be recommended. Surgery in these situations is elective, that is, the timing of such surgery is usually not an emergency that needs to be done immediately.
At other times surgery may be urgent and life-saving. The reasons for urgent surgery vary between ulcerative colitis and Crohn’s disease. People with ulcerative colitis may develop sudden, severe attacks that are not responding to any medication and may be life threatening. Severe inflammation of the colon lining may lead to massive dilation and risk of perforation (toxic megacolon). Rarely, severe life threatening bleeding may occur. Sometimes a perforation (hole in the colon) results from such severe conditions which can lead to a severe infection known as peritonitis and sepsis. These conditions require emergency surgery with removal of the colon.
It is possible that people with Crohn’s disease of the colon could experience the same conditions. If that happens, they would also need emergency surgery. However people with Crohn’s disease are more likely to have other complications which may require urgent or emergent surgery. Sometimes Crohn’s disease will cause scarring to develop, which leads to a narrowing (stricture) of the bowel. This may cause obstruction or blockage. Other people with Crohn’s disease may develop ulcers that eventually cause tunnels that lead to other parts of the intestines (large or small bowel), the bladder, the vagina or even to the surface of the skin. These tunnels are called fistulas. Surgery may be indicated if medications cannot control the tunnels. Sometimes these tunnels can lead to leakage of infection and the development of an abscess (boil). An abscess may require antibiotics and often will need to be drained. Drainage can often be done by interventional radiology via minimally invasive approaches, however, occasional surgery may be needed. Some people with Crohn’s disease will develop anal fistulas and fissures. In fact, 8-12% of people with Crohn’s disease will present with anal problems as the first sign of their disease.
Ulcerative Colitis
Most people requiring surgery for UC will be able to have elective surgery. The most common operation is proctocolectomy with ileal pouch anal anastomosis (IPAA or J-pouch), which serves a new rectum, avoiding permanent ileostomy. Actually the pouch may be shaped like a J, S, or W. Usually this is done in two stages with a temporary stoma (external bag) necessary for about 8 weeks to allow the pouch to heal. Other options for surgery for ulcerative colitis include a permanent ileostomy (a stoma with external bag to collect waste), a continent ileostomy (a stoma that does not require the wearing of a bag) and an ileorectal anastomosis. A permanent ileostomy is overall the quickest route to recovery but for many people is not very appealing due to the need for the bag. A continent ileostomy is a very complex procedure with the highest risk for revisional surgery. It is only used under very special circumstances. The ileorectal anastomosis leaves the diseased rectum in place. It is rarely used. In the case of emergency colectomy or when strong immunosuppressive drugs are being utilized (for example, Remicade, Humira, mercaptopurine or Azathioprine and steroids) it is sometimes necessary to have a three-stage approach where the first stage simply removes the colon and an ileostomy is made but the rectum is left in place. This gives time for people to heal their bodies and become healthy again before undergoing more extensive reconstructive procedures.
Crohn’s Disease
Patients with Crohn’s needing a complete colectomy are not candidates for IPAA or continent ileostomy. Because Crohn’s disease can be limited to small areas of the large and/or small bowel, it is, however, possible to take out small segments of intestine and simply put the bowel together again (bowel resection). Temporary stomas are sometimes necessary. Abscesses may need to be drained surgically and fistulas repaired surgically. Strictures can sometimes be managed without removing any bowel. Instead the stricture can simply be opened up (strictureplasty). Patients with anorectal Crohn’s disease may need specialized surgery including the use of special drains called “setons”. These drains can be left in place for many months if needed. Every attempt is made to avoid surgery for anorectal Crohn’s disease as wounds sometimes won’t heal. It is possible that surgery could lead to even more complications rather than fixing the problem.
Your Choice of Surgeon
The surgeons at The Nebraska Crohn’s and Colitis Center of Excellence have had special training in the surgical care of IBD patients and the procedures described above including the use of minimally invasive (laparoscopic) surgery. They are board certified in Colon and Rectal Surgery. Should your primary gastroenterologist determine surgery should be considered, you would be referred for more detailed discussion with a surgeon on the options available for your situation including risks associated with the surgery, anticipated functional outcome and the potential impact that a specific operation might have on your quality of life. Additional information on surgical aspects of IBD can be found at www.colonrectalsurgeons.com, www.fascrs.org and www.ccf.org.